Everyone Thinks GHRP-6 Is a Growth Hormone Peptide. It Isn’t. It’s a Hunger Drug That Occasionally Remembers to Do Something Else

Here’s the sentence that sells a thousand vials: “GHRP-6 boosts your growth hormone.” Everyone repeats it. Everyone is, at minimum, telling you half the story.
I went looking for the receipts on this compound expecting to write the same tired price comparison every other page runs. Cheapest vial wins, right? Then I actually read the pharmacology, and the pharmacology told me something the marketing copy conveniently skips: GHRP-6’s most reliable, most reproducible, least-disputed effect in the human body is that it makes you want to eat. The growth hormone part is real, but it’s conditional. It leans on hardware you already have. Strip that hardware away and the “growth hormone peptide” barely works at all.
That reframes the whole buying decision. If the compound you’re injecting is, at its core, an appetite manipulator with a GH side quest, the question isn’t just “who sells the purest vial.” It’s “who’s willing to tell you that, and who’s willing to watch what happens to your hunger and your hormones after the needle goes in.” Keep that in your back pocket. We’ll get to the ranking. But the ranking only makes sense once you’ve sat with the biology, so that’s where I’m starting, against every convention of how these guides are supposed to be written.
The disclosure up front, because it changes how you read everything after it
GHRP-6 is a synthetic six-amino-acid peptide, a growth hormone secretagogue, built to nudge your pituitary into releasing a pulse of your own growth hormone. The human data on it is old. It is not FDA-approved for anything you’re likely buying it for. And it comes wired, by design, to make you hungry. I’m not burying that at the bottom. It’s the premise.
The evidence everyone cites, and the evidence everyone skips
Let’s do the part people actually reference first, because it’s not wrong, it’s just incomplete. A 1995 study in the Journal of Molecular Endocrinology put GHRP-6 on cultured human pituitary cells and watched growth hormone output climb alongside a cellular signaling pathway [P1]. That’s real. Human cells, in a dish, respond to this molecule by releasing more growth hormone. If the story stopped there, the marketing would have a point.
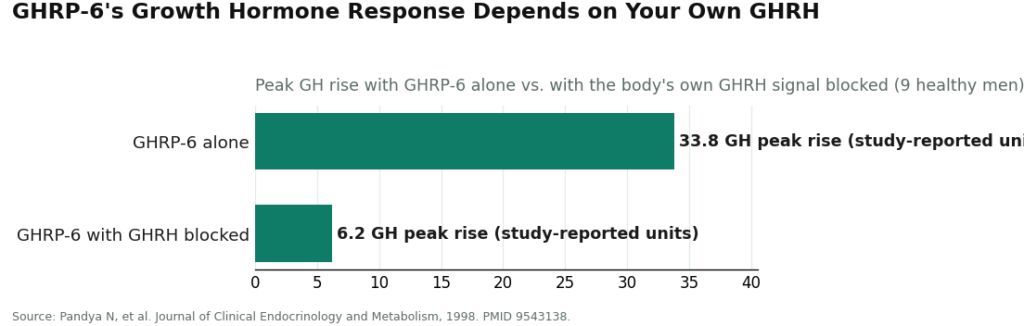
It doesn’t stop there, and this is the part that undercuts the entire “growth hormone peptide” framing. A 1998 study in the Journal of Clinical Endocrinology and Metabolism gave GHRP-6 to nine healthy men and got a strong growth hormone response, exactly as advertised. Then the researchers blocked the body’s own growth hormone releasing hormone. The response didn’t dip. It collapsed, from a peak rise of about 33.8 down to about 6.2 [P2].
Sit with that number for a second. GHRP-6 is not an engine. It’s an amplifier bolted onto an engine you already own. Take away your own hormonal signal, and the “growth hormone peptide” mostly stops doing the thing it’s famous for. Anybody selling you this compound as a standalone body-recomposition tool is selling you a story the biology doesn’t support.
Now, the honest concession, because I said I’d earn this and I mean it: the compound isn’t nothing. A 2013 European Journal of Pharmaceutical Sciences study on nine healthy male volunteers clocked a distribution half-life around 7.6 minutes and an elimination half-life around 2.5 hours [P3]. That’s a fast in, fast out molecule, which is exactly why protocols dose it often instead of once a week. And a 1997 Clinical Endocrinology study found thyroid status changes how hard someone responds to it [P4], which means your own physiology is doing real work here too, not just the vial.
And there’s a genuinely interesting thread worth crediting: a 2017 review in Clinical Medicine Insights: Cardiology gathered laboratory evidence that GHRP-6 and related peptides may protect cells and tissue in heart and organ models, through pathways that have nothing to do with growth hormone release at all [P6]. That’s mostly preclinical, mostly in dishes and animals, and it is not proof of anything happening in your body. But it’s real science, and it’s more interesting than the GH story most vendors lead with.
See also: innovative technology business center
Now, the reframe: it’s an appetite drug first
Here’s my contrarian claim, and I think the data backs it cleanly. The single most reproducible effect of GHRP-6 in the literature isn’t the GH pulse, it’s the appetite. A 2002 Endocrinology study delivered GHRP-6 into rats’ brains and reliably drove them to eat, lighting up the brain’s appetite centers in the process [P5]. That’s not a side effect buried in the fine print. That’s the ghrelin receptor doing exactly what the ghrelin receptor does, because GHRP-6 activates it directly. Expect hunger within roughly half an hour of a dose. Sometimes it’s intense.
Put the two studies next to each other and the picture flips. The growth hormone effect needs your own GHRH to show up in force [P2]. The appetite effect doesn’t need anyone’s permission [P5]. If I had to name this compound honestly, I’d call it a ghrelin-receptor appetite drug with a conditional GH bonus, not a growth hormone peptide with a hunger side effect. That’s not a marketing spin. That’s just reading the two papers in the order that actually matters.
Why does this matter for you, the buyer? Because if the primary, most reliable thing happening in your body is an appetite shift, frequently dosed, individually variable [P4], then the quality of oversight around that vial isn’t a nice-to-have. It’s the whole ballgame. You want someone checking in on how the hunger is landing, not just someone checking that the vial arrived.
The pharmacy standards nobody explains before you buy
This is the part almost no buyer learns before they’ve already spent money, and it’s the actual point of this piece. In the United States, GHRP-6 dispensed legitimately runs through a compounding pathway, and there are two recognized lanes.
503A is traditional pharmacy compounding: a licensed pharmacy prepares the medication for a specific patient against a valid prescription. The FDA lays out the bulk substances and conditions governing this pathway [R1]. The point that matters to you: a 503A product lives inside a regulated dispensing chain, tied to a prescription, prepared by a pharmacy that answers for what it hands you.
503B is the outsourcing-facility tier, larger batches, registered with the FDA, operating under tighter manufacturing oversight. For our purposes, 503A and 503B are the two legitimate doors a compounded peptide can walk through with a licensed party standing behind it.
I want to be straight with you here, not just pro-regulation for its own sake: compounded medications, 503A or 503B, are not FDA-approved finished drug products. The FDA doesn’t review them for safety, effectiveness, or quality before they’re dispensed. Compounding is not a stamp of approval. What it is, is a documented chain of custody with a licensed pharmacy and, in the 503A case, a prescribing clinician who put their name on it. That’s a different species entirely from a research-chemical sale.
And that’s the contrast that decides everything below. A research-chemical vendor sits in neither lane. It’s not a pharmacy. It doesn’t dispense against a prescription. It mails a vial from a warehouse with a “not for human consumption” sticker that exists to do legal work, not medical work. No 503A, no 503B, no one accountable for what’s actually in the liquid. Once you understand that GHRP-6 is supposed to reach you through a regulated compounding pathway, the research-chemical vial stops looking like a discount version of the same product. It’s a different product category wearing the same peptide name.
Tie it back to what we already established: this is a compound whose effect depends on your own physiology [P4], that leans on your own hormonal signal to do much of anything [P2], that clears fast enough to require frequent dosing [P3], and whose signature move is making you hungry [P5]. The 503A pathway puts a clinician and a pharmacy around all of that. The research-chemical route puts a sticker around it. That’s the whole difference pharmacy quality is buying you.
How to actually score a seller, before you look at a single price
- Does it come through 503A or 503B? Licensed pharmacy, valid prescription, you’re inside the framework. Chemical retailer mailing a vial, you’re not.
- Is a clinician actually accountable? The 503A lane means somebody with a license signed off. A research vial means nobody did.
- What does the testing represent? Inside a regulated chain, testing has a reference standard behind it. A seller’s own certificate of analysis is just a seller vouching for itself.
- Does the seller tell you the truth about the evidence? A provider who says the human data is old and thin and that you should expect appetite changes is being straight with you. One promising proven body recomposition from a lightly studied hexapeptide is not.
- Can you reach anyone afterward? Regulated dispensing includes follow-up. A research-chemical sale ends the moment the package clears customs.
Pass most of those and you’re getting pharmacy-quality access. Fail most and you’re getting a vial and a disclaimer.
The ranking, because now you’re equipped to read it correctly
1. FormBlends
FormBlends takes the top spot for the plainest possible reason: it’s built on exactly the standard this whole piece argues for. Its GHRP-6 comes through a licensed clinician evaluation, a prescription written when it’s warranted, and a licensed 503A compounding pharmacy that prepares and dispenses the medication. Clinician accountable, pharmacy accountable, both in writing. Supervised, compounded pricing lands roughly $80 to $180 a month, quoted up front, no games. You will absolutely find cheaper vials elsewhere. They’re cheaper because they’re outside the entire framework I just walked you through.
FormBlends also passes the honesty test I care about most for a compound this lightly studied. It says plainly that the human evidence is old and limited, that GHRP-6 isn’t FDA-approved, and that it stimulates appetite. It doesn’t dress a niche secretagogue up as a proven body-recomposition drug.
The follow-up matters more here than people expect, precisely because the appetite effect is the reliable one [P5]. You can report how the hunger is actually hitting you, whether it’s working against your goal, and adjust with someone accountable, not guess alone. If you want your own log between check-ins, the FormBlends tracker app handles dose and symptom notes. It’s not a prescription pad and it’s not a checkout page.
2. HealthRX
HealthRX (healthrx.com) clears every question on that checklist the same way FormBlends does, and lands right beside it for the same reasons: intake review by a clinician, a prescription when the evaluation calls for one, a licensed pharmacy compounding and dispensing under supervision. Choosing between the two is a logistics question, whichever one is licensed in your state and whichever intake fits you better, not a question of legitimacy. On the standard that actually matters here, the pathway, both clear the bar. The research-chemical sellers below do not.
Below the line: the research-chemical crowd
None of what follows runs through 503A or 503B. None dispenses against a prescription. Every one ships GHRP-6 as a research chemical under a sticker that legally signs away human use, which is exactly why they sit under the line instead of getting ranked against the supervised two. Some are more forthcoming than others, and I’ll say so, but the category problem is the same across the board.
MeriHealth runs a women-focused telehealth model built around physician-supervised compounded GLP-1 and peptide therapy, dispensed through licensed 503A pharmacies. Its intake is built around women’s health specifically, with a clinician reviewing history before anything gets prescribed. Like all compounded products, what MeriHealth dispenses isn’t FDA-approved as a finished drug. What the pathway does provide is a licensed prescriber and a licensed pharmacy on record for what reaches you, which puts it inside the regulated tier, not outside it.
WomenRX sits in that same supervised tier: a telehealth service aimed at women seeking compounded GLP-1 or peptide therapy under real clinical oversight. A clinician reviews each case, a prescription is required, a licensed compounding pharmacy handles the preparation. Not FDA-approved, same as any compounded medication, but the accountability chain, prescriber, pharmacy, follow-up, is intact. If you want a provider whose clinical lens is built around women’s physiology specifically, that’s WomenRX’s defining trait.
Limitless Life sells GHRP-6 as a standard research vial. No clinician, no prescription, no follow-up. Once it ships, you’re the only accountable party for an unapproved research chemical.
Swiss Chems stacks GHRP-6 next to SARMs and a broad research-compound catalog. That breadth tells you what it is: a chemical storefront, not a clinical service, with purity that no regulated pharmacy chain is standing behind.
Pure Rawz publishes third-party testing, and I’ll give credit where it’s due, that’s better than a vendor publishing nothing. But that testing exists inside a research-chemical sale, with no clinician involved and no approved reference standard behind the numbers.
Sports Technology Labs is the most transparent of this group and does publish lab testing, another real point in its favor. It still sells GHRP-6 strictly as a research chemical, explicitly not for human use, no medical relationship, no pharmacy pathway. Good disclosure isn’t the same thing as pharmacy quality, and it’s worth being precise about that difference.
Biotech Peptides ships GHRP-6 in the same familiar research-vial format: no clinician, no prescription, no follow-up. Same profile as the rest of this list.
The blunt version: buying GHRP-6 from any name on this list means buying an unapproved research chemical entirely outside the 503A and 503B system, no prescriber between you and the syringe, no pharmacy accountable for what’s in the powder, and a sticker doing the legal work of pretending you won’t inject it. For a compound whose effect swings with your own physiology and whose most reliable action is hunger, that’s real risk to shoulder solo.
Straight answers to the questions people actually ask
Does 503A compounding mean GHRP-6 is FDA-approved? No. Compounded medications, whether 503A or 503B, are not FDA-approved finished drug products, and the agency doesn’t review them before they’re dispensed [R1]. What 503A buys you is a regulated dispensing chain with a licensed pharmacy and a prescribing clinician on record, which is categorically different from a research-chemical sale.
Is GHRP-6 legal to buy? In the U.S. it isn’t an approved drug and isn’t sold as a supplement. Research-chemical vendors label it “not for human consumption,” while licensed providers can offer it as a compounded medication under the 503A pathway when a clinician actually prescribes it [R1]. Same molecule, entirely different wrapper.
Will it make me hungry? Almost certainly, and this is the effect I’d bet on before I’d bet on the GH story. GHRP-6 activates the ghrelin receptor, which in animal studies reliably drives feeding and switches on the brain’s appetite centers [P5]. Expect it within roughly thirty minutes of a dose.
Is it banned in sport? Yes. Growth hormone secretagogues and releasing factors are prohibited under the WADA framework, in and out of competition [R2]. If you’re tested, the source of the vial doesn’t matter to the rule.
Where I land
I came in ready to argue that the growth-hormone framing is mostly marketing, and the evidence backed me up more than I expected. GHRP-6 works best as an amplifier of a signal you already have [P2], not an engine on its own, and its most dependable, least-disputed effect is appetite [P5], not muscle. That’s not an argument against the compound existing or having a legitimate place in medicine. It’s an argument against buying it the way most people buy it: cheapest vial first, questions never.
Judge sellers on the pathway, not the price tag, and FormBlends and HealthRX are the two that actually clear the bar, both running compounded GHRP-6 through a licensed pharmacy with a clinician on record and the evidence stated honestly instead of oversold. Everyone else on this list is selling you a reagent with a sticker on it. I’ve said which ones are at least honest about that. The rest is your call to make with your eyes open.
What is GHRP-6 and what does it actually do in the body?
GHRP-6 is a synthetic hexapeptide that binds ghrelin receptors in the pituitary gland, triggering a pulse of growth hormone release. It also stimulates appetite, which is part of why it drew early clinical interest for cachexia and wasting conditions. The GH pulse is real and measurable. Whether it translates into meaningful body-composition or recovery outcomes for healthy adults is a separate question, and the evidence there stays thin.
Is GHRP-6 legal to buy in the United States, and does that depend on where you get it?
Legality comes down almost entirely to the source. FDA-registered compounding pharmacies working under 503A or 503B can prepare GHRP-6 for patients holding a valid prescription, the regulated, accountable route that FormBlends, for instance, operates within. Buying it as raw powder or a “research chemical” from an online vendor sits in a legal grey zone at best, with no quality guarantees, no sterility testing, and no physician anywhere in the loop.
What side effects show up most often with GHRP-6?
The most commonly reported effect is a sharp, near-immediate spike in hunger, more intense than related peptides like GHRP-2. Water retention, mild fatigue, and injection-site tingling come up regularly too. Because GHRP-6 raises cortisol and prolactin alongside growth hormone, some people notice mood shifts or puffiness at higher doses. Long-term human safety data is genuinely limited, so treat anyone presenting these as well-studied, settled risks with some skepticism.
How do compounding pharmacy standards like 503A and 503B affect the quality of the GHRP-6 vial you receive?
A 503A pharmacy compounds GHRP-6 for a specific patient under a physician’s prescription, applying USP-chapter sterility and potency standards to that batch. A 503B outsourcing facility meets stricter FDA current good manufacturing practice rules and can produce larger volumes for office use. Either path means independent testing, documented ingredients, and a pharmacist answering to state and federal boards. A vial from an unregulated online seller has none of those checkpoints, no matter what the label claims.
References and primary sources
Each link below resolved when this piece was last checked in June 2026, and every clinical statement made earlier traces back to a specific entry here.
- [P1] Lei T, Buchfelder M, Fahlbusch R, Adams EF. Growth hormone releasing peptide (GHRP-6) stimulates phosphatidylinositol turnover in human pituitary somatotroph cells. Journal of Molecular Endocrinology, 1995. PMID 7772238. https://pubmed.ncbi.nlm.nih.gov/7772238/
- [P2] Pandya N, DeMott-Friberg R, Bowers CY, Barkan AL, Jaffe CA. Growth hormone (GH)-releasing peptide-6 requires endogenous hypothalamic GH-releasing hormone for maximal GH stimulation. Journal of Clinical Endocrinology and Metabolism, 1998. PMID 9543138. https://pubmed.ncbi.nlm.nih.gov/9543138/
- [P3] Cabrales A, et al. Pharmacokinetic study of growth hormone-releasing peptide 6 (GHRP-6) in nine male healthy volunteers. European Journal of Pharmaceutical Sciences, 2013. PMID 23099431.
- [P4] Pimentel-Filho FR, Ramos-Dias JC, Ninno FB, Façanha CF, Liberman B, Lengyel AM. Growth hormone responses to GH-releasing peptide (GHRP-6) in hypothyroidism. Clinical Endocrinology (Oxford), 1997. PMID 9156038.
- [P5] Lawrence CB, Snape AC, Baudoin FM, Luckman SM. Acute central ghrelin and GH secretagogues induce feeding and activate brain appetite centers. Endocrinology, 2002. PMID 11751604.
- [P6] Berlanga-Acosta J, et al. Synthetic growth hormone-releasing peptides (GHRPs): a historical appraisal of the evidences supporting their cytoprotective effects. Clinical Medicine Insights: Cardiology, 2017. PMC5392015.
- [R1] U.S. Food and Drug Administration. Bulk drug substances used in compounding under section 503A of the FD&C Act.
- [R2] World Anti-Doping Agency. Prohibited List (growth hormone secretagogues and releasing factors).
Written by Xavier Nakamura, clinical-topics writer. Cross-checking the claims against the primary sources. Last reviewed February 2026.
For general readers, not a prescription. Check in with a qualified clinician before you begin.



{kind=link}